Splenic silicosis, a rare extrapulmonary manifestation of occupational silica exposure: A case report
Keywords:
Silicosis, Silica, Lung diseases, Occupational exposure, RadiographyAbstract
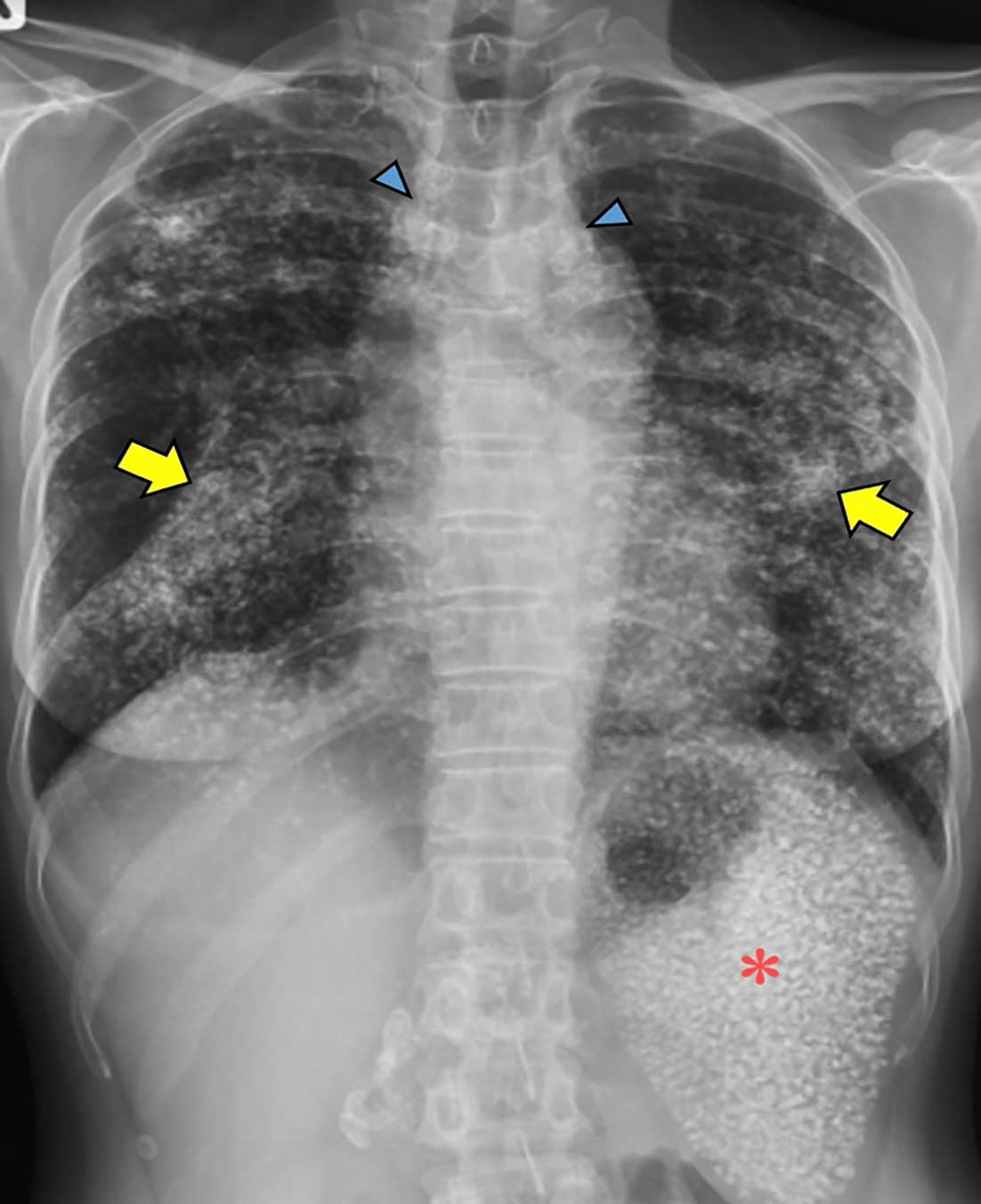
Introduction: Silicosis is a well-recognised occupational lung disease caused by inhalation of crystalline silica dust; however, extrapulmonary involvement, particularly splenic silicosis, remains rare and underreported in the literature.
Case presentation: A 46-year-old female sand sifting machine operator presented with six years of occupational silica exposure at a sand classification and packing factory. In 2005, she developed respiratory symptoms, and chest radiography revealed diffuse nodular opacities, although silicosis was not diagnosed at that time. In October 2024, approximately 19 years after initial presentation, computed tomography demonstrated multiple calcified pulmonary nodules, progressive massive fibrosis, eggshell calcification of mediastinal lymph nodes, and multiple calcified micronodules throughout the splenic parenchyma. Based on these characteristic radiological findings and her occupational exposure history, a diagnosis of complicated silicosis with extrapulmonary splenic involvement was established. Despite a latency period shorter than the traditionally reported 10–30 years for chronic silicosis, the clinical course was indolent across the interval between the two assessments (2005 and 2024), which may lie near the boundary between chronic and accelerated forms.
Conclusions: Splenic silicosis should be considered in patients with occupational silica exposure who present with splenic calcifications. Although sand sifting operations have received limited attention as a potential source of silica exposure, the occurrence of multiple cases at the same facility suggests potentially high exposure intensity. These findings emphasise the importance of comprehensive prevention strategies and raise the question of whether earlier initiation of health surveillance may benefit workers in sand processing industries.
References
1. Leung CC, Yu IT, Chen W. Silicosis. Lancet 2012; 379(9830): 2008-18
2. Yang B, Liu X, Peng C, Meng X, Jia Q. Silicosis: from pathogenesis to therapeutics. Front Pharmacol 2025; 16: 1516200
3. Pollard KM. Silica, silicosis, and autoimmunity. Front Immunol 2016; 7: 97
4. Slavin RE, Swedo JL, Brandes D, Gonzalez-Vitale JC, Osornio-Vargas A. Extrapulmonary silicosis: a clinical, morphologic, and ultrastructural study. Hum Pathol 1985; 16(4): 393-412
5. Carreño Hernández MC, Garrido Paniagua S, Colomés Iess M, Guemra M. Accelerated silicosis with bone marrow, hepatic and splenic involvement in a patient with lung transplantation. BMJ Case Rep 2019; 12(12): e230781
6. Eide J, Gylseth B, Skaug V. Silicotic lesions of the bone marrow: histopathology and microanalysis. Histopathology 1984; 8(4): 693-703
7. Yang HS, Kim JI, Ye BJ, Yoo TJ, Lee SW, Jung KY. A case of complicated silicosis with a complex clinical course in a glass manufacturing worker. Ann Occup Environ Med 2014; 26: 10
8. Vanhoenacker FM, Van den Brande P, De Schepper AM. Hepatosplenic antracosilicosis: a rare cause of splenic calcifications. Eur Radiol 2001; 11(7): 1184-6
9. Shen TC, Chen CH. Silicosis with splenic involvement. QJM 2013; 106(1): 89-90
10. Yatera K, Ono S, Joko K, Mukae H. Splenic calcification in a patient with silicosis. Intern Med 2015; 54(8): 987-8
11. Bai M, Dwivedi DP, Babu VM, Warrier LS, Chauhan AS. Splenic silicosis: a rare cause of splenic calcifications. Indian J Occup Environ Med 2021; 25(3): 185-7
12. Ufuk F. Calcified splenic lesions: silicosis and systemic lupus erythematosus should be considered in the differential diagnosis. AJR Am J Roentgenol 2020; 215(6): W63
13. Consul N, Javed-Tayyab S, Lall C, Jensen CT, Menias CO, Pickhardt PJ, et al. Calcified splenic lesions: pattern recognition approach on CT with pathologic correlation. AJR Am J Roentgenol 2020; 214(5): 1083-91
14. International Labour Office. Guidelines for the use of the ILO international classification of radiographs of pneumoconioses. Revised edition 2022. Geneva: International Labour Office; 2022
15. Dixit R, Arya MK, Panjabi M, Gupta A, Paramez AR. Clinical profile of patients having splenic involvement in tuberculosis. Indian J Tuberc 2010; 57(1): 25-30
16. Lee WK, Van Tonder F, Tartaglia CJ, Dagia C, Cazzato RL, Duddalwar VA, et al. CT appearances of abdominal tuberculosis. Clin Radiol 2012; 67(6): 596-604
17. Yates DH, Johnson AR. Silicosis and other silica-related lung disorders. In: Feary J, Suojalehto H, Cullinan P, editors. Occupational and Environmental Lung Disease. Sheffield: European Respiratory Society; 2020. p. 150-75.
18. Tangsurased K, Dumavibhat N, Chansaengpetch S, Virojskulchai T, Bunman S, Ingviya T, et al. Chronic silicosis as the potential consequence of short-term exposure to silica: a case report. BKK Med J 2024; 20(1): 29-32
19. Dumavibhat N, Matsui T, Hoshino E, Rattanasiri S, Muntham D, Hirota R, et al. Radiographic progression of silicosis among Japanese tunnel workers in Kochi. J Occup Health 2013; 55(3): 142-8
20. Salum KCR, Castro MCS, Nani ASF, Kohlrausch FB. Is individual genetic susceptibility a link between silica exposure and development or severity of silicosis? A systematic review. Inhal Toxicol 2020; 32(9-10): 375-87
21. Hoy RF, Dimitriadis C, Abramson M, Glass DC, Gwini S, Hore-Lacy F, et al. Prevalence and risk factors for silicosis among a large cohort of stone benchtop industry workers. Occup Environ Med 2023; 80(8): 439-46
22. U.S. Environmental Protection Agency. AP-42, Compilation of Air Pollutant Emission Factors. Section 11.19.1: Sand and Gravel Processing. Research Triangle Park, NC: Office of Air Quality Planning and Standards; 1995
23. Wills BA, Finch JA. Wills’ Mineral Processing Technology: An Introduction to the Practical Aspects of Ore Treatment and Mineral Recovery. 8th ed. Oxford: Butterworth-Heinemann; 2016
24. Sanderson WT, Steenland K, Deddens JA. Historical respirable quartz exposures of industrial sand workers: 1946-1996. Am J Ind Med 2000; 38(4): 389-98
25. Fazio JC, Viragh K, Houlroyd J, Gandhi SA. A review of silicosis and other silica-related diseases in the engineered stone countertop processing industry. J Occup Med Toxicol 2025; 20(1): 9
26. Youngchaiyud P, Dumavibhat N. Evaluation of pulmonary impairment. In: Workmen’s Compensation Fund Office, Social Security Office, editor. Manual for the assessment of permanent physical and mental impairment. 4th electronic ed. Bangkok: The Office; 2021. p. 593-622.
Downloads
Published
Issue
Section
License
Copyright (c) 2026 The Author(s)

This work is licensed under a Creative Commons Attribution-NonCommercial 4.0 International License.
Mattioli 1885 has chosen to apply the Creative Commons Attribution NonCommercial 4.0 International License (CC BY-NC 4.0) to all manuscripts to be published.
How to Cite



